
The COVID Uncoupling
The COVID Uncoupling
This is not the pandemic we started with.


There was a good article in the New York Times recently on the topic of how COVID cases are surging, but COVID deaths remain low. This is a phenomenon often referred to as “uncoupling,” meaning essentially that catching COVID is not linked (“coupled”) as strongly with severe outcomes like hospitalization and death. I think this is an important trend, and it points to a path forward and out of the pandemic.
In this article, I give a bit more background on the numbers and the uncertainty surrounding them, as well as offer one physician’s perspective on what it means. Is there a line we can draw between decoupling and the end of the pandemic phase? I’ll explain why I believe that to be the case.
What is the Rate of COVID Cases?
I use the graphs from Our World in Data for cases and hospitalizations. They license their work freely, indicate sources, and have very slick graphics. Here’s their most recent graphic for COVID cases in the U.S.:
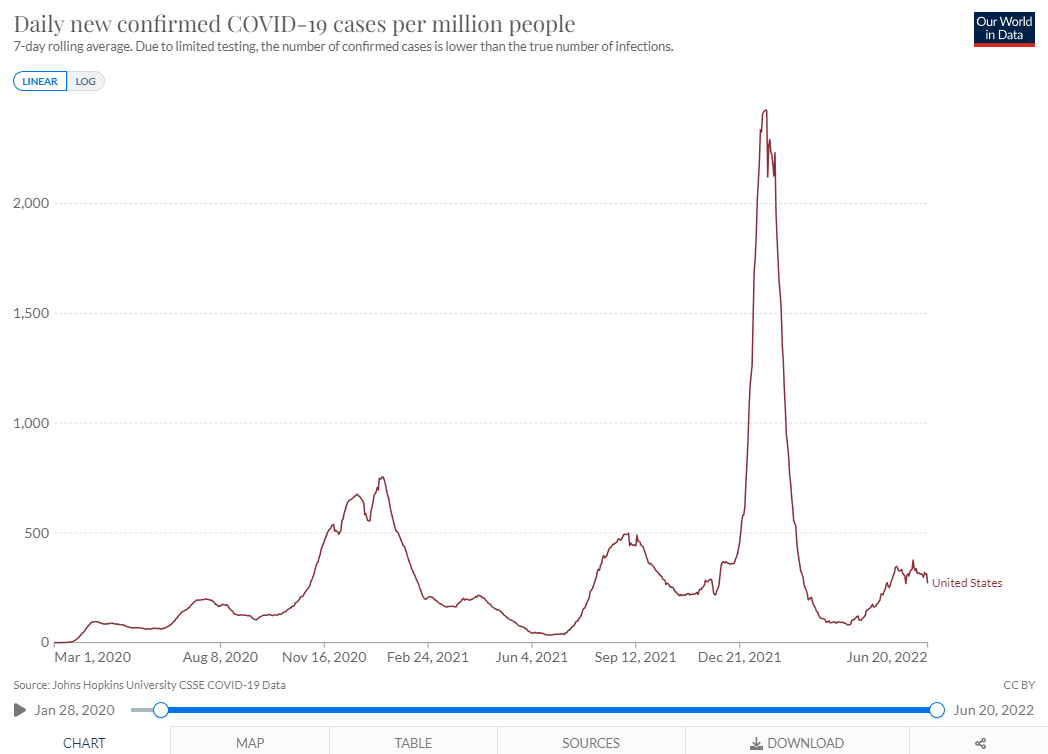
You can see the big surges, including the initial wave, the first big variant, Alpha, in 2020-2021, the Delta wave in late 2021, the holy $#!* Omicron wave from the beginning of 2022, and it recent sub-variant, the current BA.2.12.1 wave. This seems pretty clear in terms of cases, and I don’t think anyone disputes that Omicron had a huge case count. However, it must be pointed out that tests were not readily available in the beginning of the pandemic, resulting in an undercount. In contrast, testing has often been done with over-the-counter home kits in the most recent wave, and those are not generally reported officially, leading to an underestimation of total infections at the beginning and end of the pandemic.
The percentage of tests that are positive corrects somewhat. This metric doesn’t vary with the number of tests, measuring only the fraction of reported tests that were positive. In times with a lot of circulating COVID, it is more likely that any given person with symptoms who gets tested will have it, so it is a good hdge against variation caused by changes in testing approach.
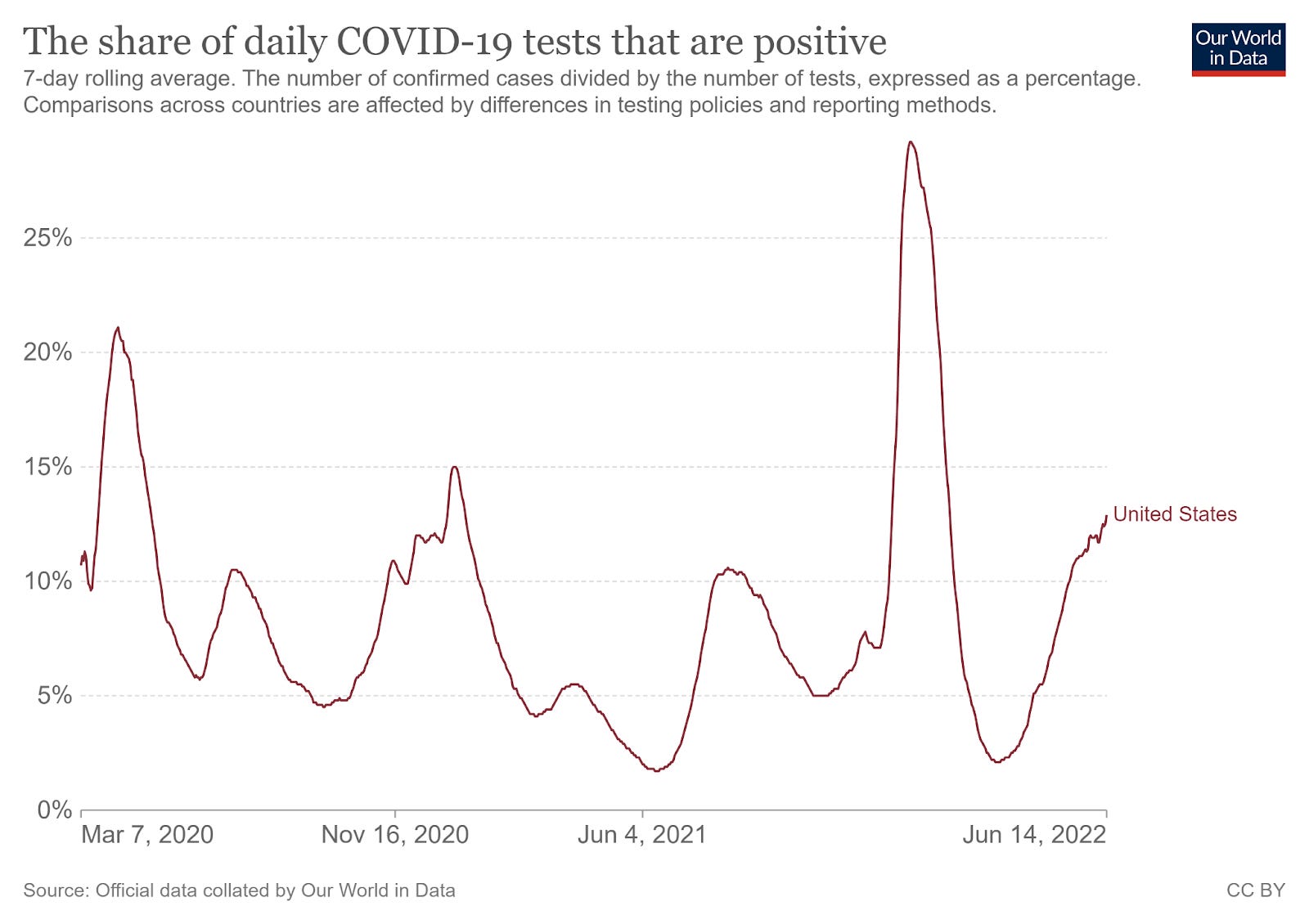
This is closer to apples-to-apples comparison across the waves. You can see that, compared to total positive cases, the test-positivity rate results in higher peaks for the beginning of the pandemic (when testing was hard to come by) and the most recent, home-test era. The Omicron peak is still huge, but now you see that our current wave may be on par with earlier ones.
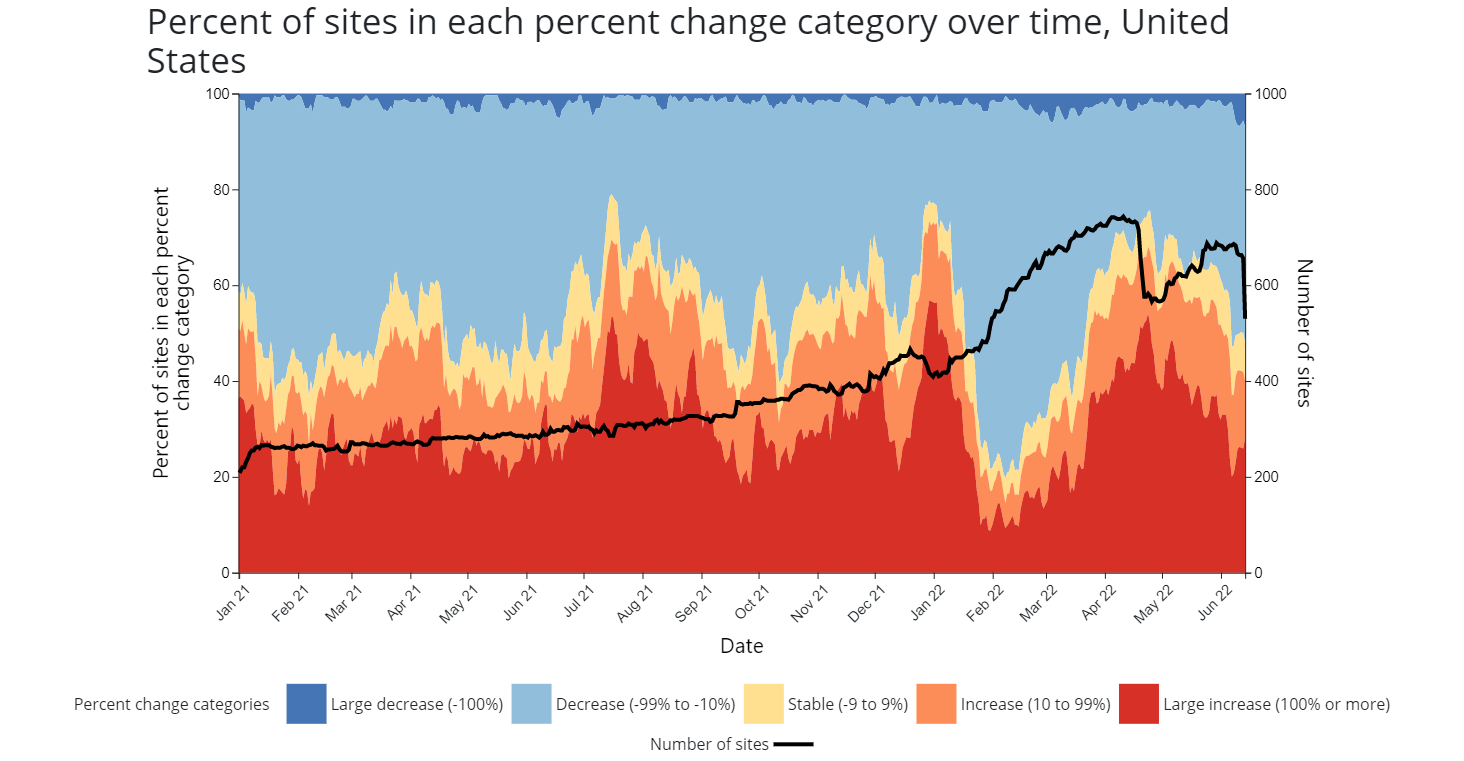
One final way of looking at the spread of COVID that eliminates the testing question entirely is to look at wastewater surveys. This is a very promising technique in the sense that it does not depend on the general public to do anything other than use the toilet. Testing the amount of COVID that passes into the sewers also shows a similar pattern of peaks. The biggest limitation on this testing type is that it is a strategy that has only been gradually rolling out. It tends to skew toward the Midwest and Northeast, with fewer reporting cities in the South and West.
This is a different way of looking at the question. It is less dependent on whether or not the cases caused enough symptoms for a person to seek testing or treatment. The red peaks are when reporting locations saw a 100% increase in COVID shedding, and you see an interesting phenomenon. In terms of shed virus, the most recent wave, March 2022 to current, is broader and almost as tall as the Omicron wave. This could be an artifact of having 50% more cities reporting (the black line), but it seems hard to pin it all on that. These numbers suggest that, at least in terms of COVID in the sewer system, the current wave is closer to Omicron than the test positivity rate would suggest. How is that possible? One answer could be a higher percentage of infections that were so mild the infected person never sought testing at all.
What is the COVID Complication Rate?
This is why we care about COVID. When it first hit, and the hospitalizations and deaths skyrocketed, we had an immediate sense of how deadly a new disease can be to a population that has never before been exposed to it. We have learned a lot since then. We learned that there is a very steep age gradient for mortality. This means that older patients are much more likely to die from a COVID infection than the young. We also learned better management techniques, such as reducing the complications associated with mechanical ventilation, and, importantly, we developed vaccines and treatments. The vaccinations are of great benefit in terms of protecting the most vulnerable from severe complications. (Note: Without totally sidetracking this article, I remain pro-vaccine, anti-mandate. I think it is appropriate to look at your individual medical risk, and your history of prior infection and make your own decision accordingly. I take care of cancer patients. I have been vaccinated and recommend vaccination to my patients.) In short, there are medical reasons why people are more likely to survive or succumb to COVID.
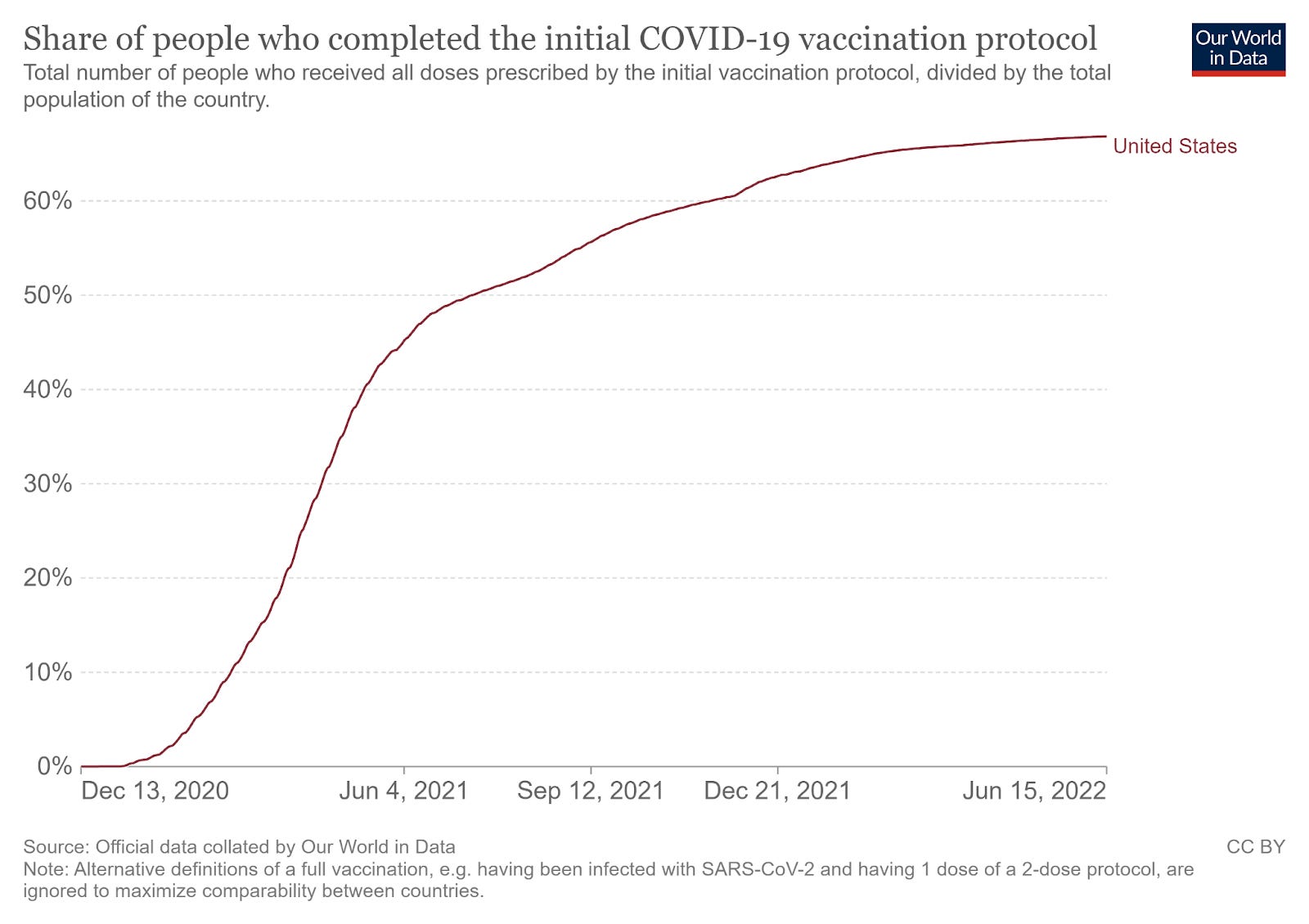
But that is not the only thing in play. It is important to emphasize that exposures to the COVID virus can induce immunity. This can be through mRNA vaccine, a modified virus vaccine, or following recovery from infection. All of these reduce the risk of future COVID, and they are to some degree additive. When you look at the vaccine uptake chart for the US, you see that, while it has plateaued, a majority of the population are fully vaccinated.
Vaccination is one way to develop resistant to a virus. Recovering from infection is another. The CDC tries to estimate how many Americans have been infected by using tests for COVID antibodies in the blood serum. This is a separate test from vaccine-induced antibodies. The most recent estimate was through February, at which time roughly 58% of Americans and about 75% of kids 17 and under showed evidence of prior infection. That percentage was going up on average by 1-2% per week.
Data out of Israel and published in the New England Journal of Medicine showed evidence of persistent, albeit waning, immunity after either type of exposure. In that study, the combination of vaccine and prior infection provided the most durable protection, followed by prior infection, then two doses of mRNA vaccine. A third dose of vaccine (“booster”) looked promising for restoring immunity, but the follow-up was too short to make a valid comparison to the other approaches.
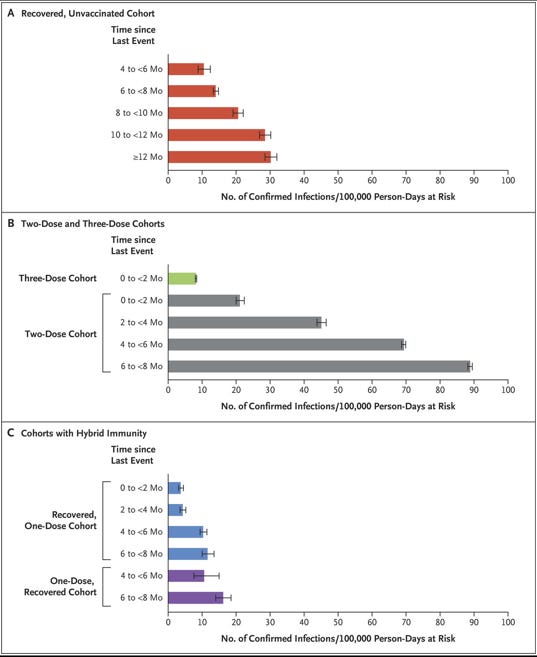
I don’t know of any good data on the percentage of Americans with hybrid immunity, but it is likely quite common. Just as important, the percentage of Americans with at least some type of protection is quite high. If the rate of prior COVID infection was 58% in February and rising by 1-2% week, a conservative estimate would have it at around 70% by now. At least 66% of the population are vaccinated. That means that, if these two phenomena (vaccination and infection) were randomly distributed, we’d have only 10% of the population with neither type of protection. It’s almost certainly even lower than that, though, because the infections tend to be more common in the unvaccinated. In the CDC’s seroprevalence study, the kids (at that time ineligible for vaccination) had a 75% prior infection rate back in April (meaning kids now are probably closing in on 90% prior infection). The bottom line, between treatment and immunity, there is a lot more protection now than there was at the start of the pandemic.
Does Protection Matter?
Short answer: yes.
But again, let's look at the data. I like to use hospitalization data, not because it is without flaws, but because it has been the most consistently collected. Standard procedure is to test patients for COVID when they are admitted. This does mean that we tend to overcount COVID as a cause of hospitalization, and it also may skew the rates higher in later months, as testing has become more available. Another issue is that one can’t look at the top level of data and know if a person was admitted with versus for COVID. It is possible (probable, in my opinion) that the percentage of with COVID (meaning COVID was an incidental finding unrelated to their reason for admission) has been rising. Even with these limitations, I think the pattern is very interesting. Let’s look at the hospitalization rates for COVID.
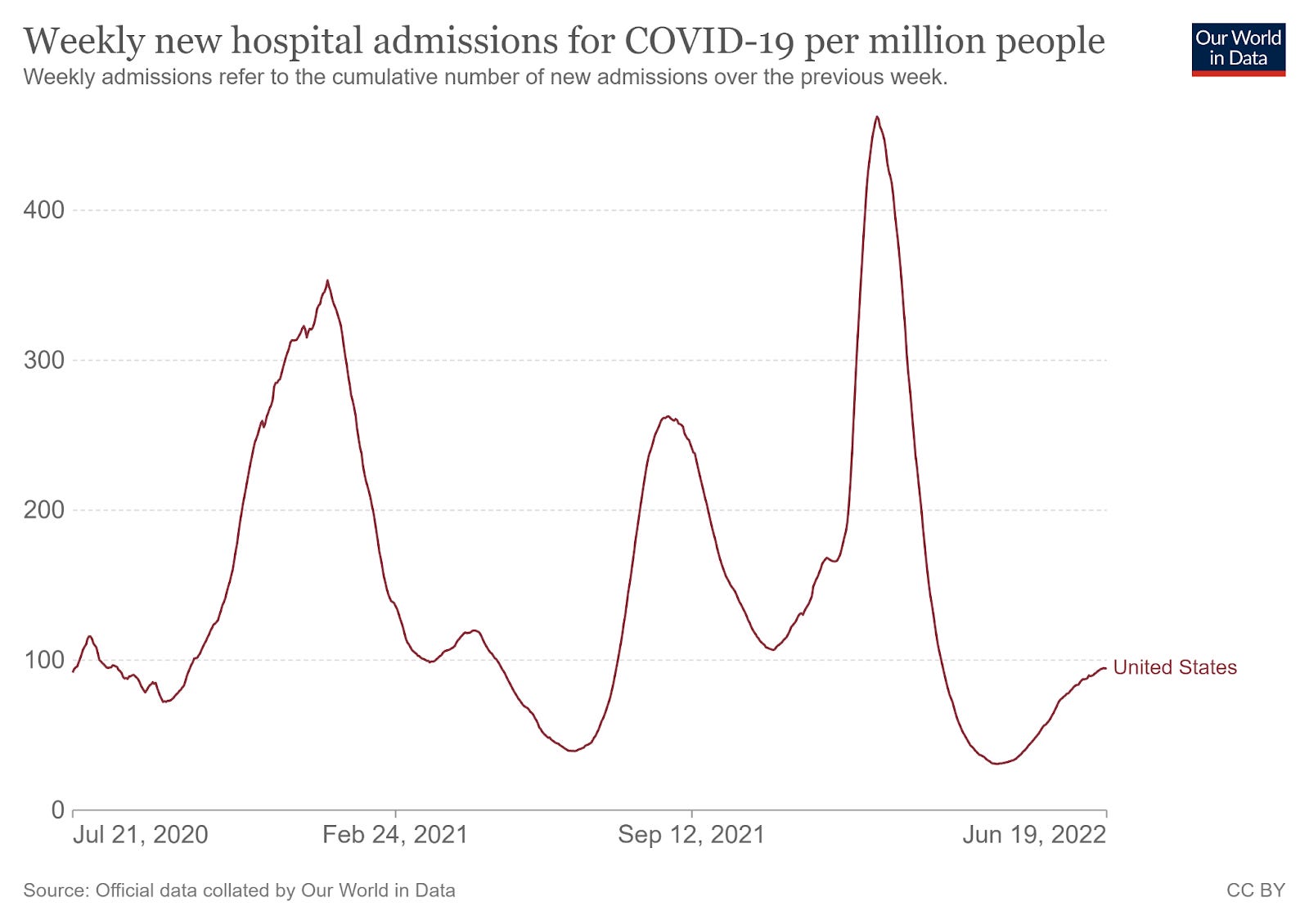
To make the comparison easy, I will reprint the test-positive rate below:
What jumps out?
1. We don’t have hospitalization data in the chart for the initial wave. it would undoubtedly be sky high, but we did not have testing resources available.
2. In early waves, the peaks for hospitalization are higher than the peak for cases in the corresponding wave. With Omicron, the peaks are about equal, and with the latest wave, the peak for hospitalization is much lower.
In other words, COVID is increasingly less likely to land a person in the hospital on a per-case basis.
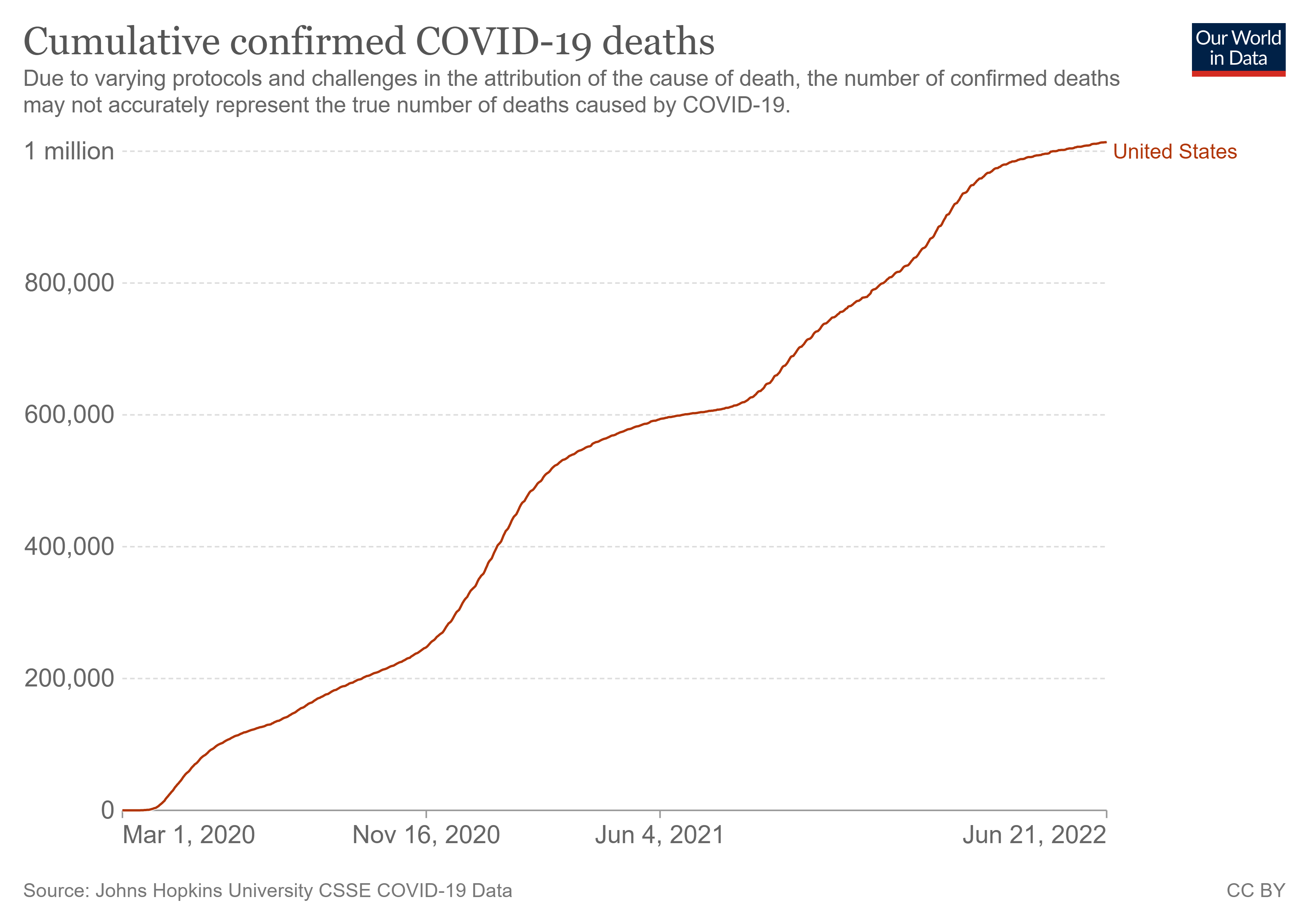
What about deaths? The data for died from COVID versus died with COVID are, if anything, a bigger mess than the hospitalization data. But there is the advantage in this set of information of having numbers from the first wave of infection.

We see a very similar pattern. In the first part of the pandemic (almost entirely people with no prior infection and vaccine not yet available) the death peaks are relatively big compared to the case peaks (remember, we had trouble counting cases early). Most recently, death peaks are similar in magnitude to cases (Omicron) and then much lower (current). In other words, the same pattern is holding. What started out as a very deadly disease in an immune-naive population is causing far fewer problems in a population that has had one or more exposures.
4. You Promised You Would Say What This all Means.
I am going with “cautious optimism.”
It is still possible that this trend could somehow reverse. There could be a variant that is so dramatically different that it evades post-vaccination, post-infection, and hybrid immunity. I don’t think that is likely. Nor, for that matter, do I think there is anything we can do about it, since by definition such a variant evades all of our current prevention strategies (and no, we will not be fighting the Mask Wars in this article). As such, I can’t see making policy based on such a hypothetical.
I believe it also takes the impetus out of any campaign to mandate vaccination. We have seen that fairly high levels of vaccination and prior infection are not preventing the current surge, which wastewater data suggest may be on par with Omicron in frequency, if not severity. I was never a fan of mandating the COVID vaccination, so you know my prior position. Vaccination has not prevented community spread, but it has protected vulnerable individuals. I think public health efforts should be directed at those who remain unvaccinated and at high risk. Talk to them (not at them) and see what their reasons are. I have found that, one on one, most people have their particular values that led them to a decision. Hear them out and they will usually do the same for you. It might change some minds and rebuild some bridges.
And finally, is this the Pandemic Exit Sign? Has the virus become so common and so mild that it has become something close to seasonal influenza? Have we reached “endemic” COVID? This is hard to define, since there are some people who will retain higher risk, even after vaccination. However, we now have medications for prevention (Evusheld) and treatment (Paxlovid) in addition to the vaccination.
There is no doubt COVID has been devastating. The chart for cumulative deaths bears that out. But if you look at the deaths in the past 3 months, the monthly rate would be about 50,000 deaths over a 6-month flu season. Bad, but not out of the range of recent experience.
So I would say we are indeed at that point. Individuals will still need to make their own risk decisions, and sadly, just like with influenza, there will be people who succumb. The question of ‘long COVID’ and what it represents, how frequent, etc, is for another day. And really, these same issues apply. Despite everything that was done, we mostly all still got COVID. Nobody is signing up to do lockdowns again with no new tools and a much more nebulous disease.
All that said, I really can only muster two cheers for the off ramp, not a full three, even if I am optimistic about the end of the pandemic. For one thing, trust in public health is at an all-time low. And whatever we think about long COVID, the effects of “long Lockdown” may turn out to be even worse, especially for kids. In other words, we have a tremendous way to go to dig out of this. Sides that have argued (raises hand) and at times generated “more heat than light” will need to find a way to come together and rebuild.
The post-pandemic phase will be a long and hard road.
It’s time we got started on it.
Cheers, y’all.
David
Great article - to me it points to the obvious, while there are no certainties in life (only probabilities), it looks like the COVID “emergency” is definitely over.